Canine Ehrlichiosis is a tick borne, febrile, debilitating disease of dogs and wild canidae caused by Ehrlichia canis transmitted by the brown dog tick Rhipicephalus sanguineus. The infections are known to occur worldwide. The disease is also known as canine typhus, canine haemorrhagic fever, tracker dog disease, idiopathic haemorrhagic syndrome and tropical canine pancytopaenia. In Kenya the disease is locally known as Nairobi bleeding disease. The disease was first discovered by Donatien and Lestoquardin 1935 at the Pasteur Institute in Algeria. They noted that experimental dogs infected with brown dog ticks developed severe febrile illness characterized by anaemia. Blood smears of infected dogs stained by Giemsa stain showed small Rickettsia-like organism inside canine monocytes. They called the newly discovered organism Rickettsia canis. In 1945 Moshkovski renamed the organism as Ehrlichia canis in honour of Paul Ehrlich the famous German Bacteriologist.
Ehrlichia are obligate intracellular bacteria which differ from rickettsiae because they replicate in the phagosome of host cell whereas all Rickettsia, with one exception (C. burnetti) grow free within the cytoplasm. Other distinguishing characters include their ultrastructure, tropism for circulating leukocytes and antigenic composition. All ehrlichiae are presumed to be tick borne and only one species, Ehrlichia sennetsu is thought to be pathogenic to humans.
Since its discovery, reports indicate that the disease has been increasing in frequency and importance. In the US the disease was first described in 1962in Oklahoma. The potential impact of the organism was greatly appreciated only in 1968, during a serious epizootic of highly fatal haemorrhagic disease called tropical canine pancytopaenia (TCP) among sentry dogs used by US troops stationed in Vietnam. The disease was characterized by general debilitation, epistaxis, anaemia and leukopaenia. Later Huxsoll in 1970 detected ehrlichial inclusions in the blood and tissues of dogs with TCP and realized that TCP was a severe form of canine ehrlichiosis.
Morphology
E. canis and other members of the genus ehrlichia are minute gram-negative cocci that stain dark blue to purple with Romanowsky stain and with Machiavello method they stain light red and brown-black with silver stain. Like Chlamydia, ehrlichia go through three developmental stages:
Elementary bodies – Individual Ehrlichia organisms
Initial bodies – Immature organismal inclusions
Morula – Mature organismal inclusions
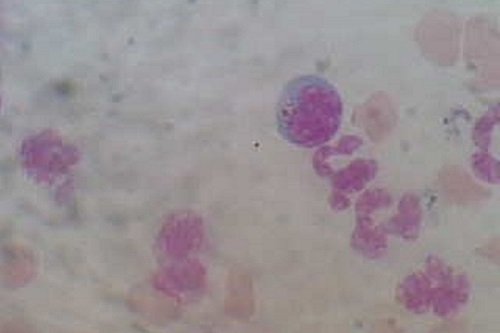
Elementary bodies are small gram-negative organisms about 0.2-0.5 µm in diameter and difficult to detect by light microscopy. Elementary bodies are usually coccoid or ellipsoidal. Elementary bodies enter canine monocytes by phagocytosis. Phagolysosomal fusion does not occur in infected cells and elementary bodies begin to grow and divide within the confines of the phagosome. Replication of organism occurs by binary fission. At 3 -5 days after infection, small members of tightly packed elementary bodies 1.0-2.5 µm in diameter are observable as pleomorphic inclusions, called as initial bodies. During next 7-12 days, additional growth and replication occurs and initial bodies develop to mature inclusions called mulberry or morula (4-6 µm in diameter). Infected monocytes usually contain several morulae each containing several dozen elementary bodies. Morula breaks up into elementary bodies when infected cell ruptures and infectious cycle is repeated. All the three growth stages occur within a membrane-lined vacuole of host origin that separates individual organisms or a group of these from the host cell cytoplasm.
Epidemiology
As early as 1935 the brown dog tick Rhipicephalus sanguineus was considered to be the vector of E. canis. Studies conclusively proved trans-stadial transmission where in larvae, nymphs and adults are able to transmit the disease. In infected ticks E. canis multiplies within haemocytes and cells of the salivary gland. Then organism enters digestive tract and infects midgut epithelium. Ticks could transmit E. canis for 155 days. Attraction of mononuclear cells to the inflamed site of tick bite may facilitate the infection of blood monocytes. Amblyomma americanum and Otobius megnini were most recently described as potential vectors. And domestic canids are currently considered the naturally susceptible to infection. Usually, the infection is sporadic and is of worldwide occurrence. Even though disease occurs in all breeds of dogs. German shepherds are most susceptible. All ages are affected, but males are found to be more affected.
Pathogenesis
Pathogenesis depends on the strain of organism, breed of dog affected, concomitant diseases and the host defense mechanism. The most common finding in an acute E.canis infection is the extensive invasion of parenchymal organs and perivascular cuffing by plasma cells particularly lungs, meninges, kidneys and spleen suggesting an immunopathologic etiology. Lymphocytes of infected dogs exert a cytotoxic effect upon autologous monocytes. Leukopaenia along with a highly prominent thrombocytopenia is a pathognomonic haematologic manifestation for canine ehrlichiosis.
Clinical disease
After an incubation period of 10-15 days canine ehrlichiosis begins as an acute febrile disease. The first stage is characterized by fever 40-41.4ºC, depression, anorexia, weight loss, oculonasal discharge, conjunctivitis, occasional vomiting and lymphadenopathy. Oedema of limbs and ataxia may also be present. The acute phase typically last for 2 or 3 weeks. Most dogs survive acute phase followed by a subclinical phase lasting several months. Animals remain infected but are generally asymptomatic and blood values remain subnormal. Characteristic features of TCP are occasional fever, corneal opacity, regenerative or non-regenerative anaemia with severe leukopaenia and thrombocytopenia. Initially there may be bone marrow hyperplasia followed by hypoplasia due to the exhaustion of cellular elements in the bone marrow. The outcome of the third and the terminal phase depends on the breed of the dog. Beagles, for example, may become chronic carriers. German shepherds usually succumb. Clinical manifestations include fever, anorexia, severe weight loss, marked pancytopaenia, anaemia and peripheral oedema. Ecchymosis and petichiae commonly occur at multiple sites. Unilateral or bilateral epistaxis is common. Death occurs due to extensive mucosal or serosal haemorrhage or due to secondary bacterial infection prompted by the dog’s debilitated condition. Increased ESR and prolonged bleeding time is very characteristic. Dogs are also susceptible to infection with E. equi and E. risticii which is mild and inapparent.
Diagnosis
A diagnosis of acute ehrlichiosis is by microscopic detection of organism in Giemsa-stained blood smears or buffy coat preparations. The morular rosettes take a light blue or lilac tint within the cytoplasm of the monocytes. The first drop of blood from a prick incision on the ear of dog is considered ideal. Percentage of infected monocytes within the peripheral blood is extremely low and hence best results are obtained by searching the feather edge of the stained whole blood smear.
An iFAT is currently the only available specific means for detection and titration of antibodies to E. canis. The organism generated by the in vitro culture techniques serves as the antigen for the test. This test can also be used for assessing the efficacy of treatment.
Treatment
Among all therapeutics tested, tetracyclines are the most effective for the treatment of E. canis and other ehrlichial infections of dogs.
First line antibiotics:
Tetracycline 22mg/kg BW IV for 14 days.
Oxytetracycline 25mg/kg BW PO TID for 21 days.
Doxycycline 5mg/kg BW PO BID for 14 days.
Minocycline 20mg/kg BW PO BID for 14 days.
Second line antibiotics:
Chloramphenicol 50mg/kg BW PO TID for 21 days.
Imidocarb dipropionate 5mg/kg BW IM or SC single injection and repeated in 2-3 weeks.
Following treatment with tetracycline, dogs in early stages of disease show spontaneous clinical and haematological improvement. Chronically infected dogs may respond more slowly to treatment. Some dogs may require prolonged treatment. Efficacy of treatment can be judged from the IFA titres. Various supportive therapies like blood transfusion using whole blood or platelet rich plasma and polyionic fluids are recommended. Short term administration of anti-inflammatory and immunosuppressive compounds may be useful for secondary immune mediated complications.
Prevention and Control
The only preventive therapeutic measure for canine ehrlichiosis is administration on a continuous basis tetracycline at a low dosage of 6.6 mg/kg/day. This can be tried in dogs travelling in enzootic area. Routine use of acaricides and control of ticks is recommended. All new dogs should be free of tick infestation and serological status screened before introducing them to E. canis free groups.
| The content of the articles are accurate and true to the best of the author’s knowledge. It is not meant to substitute for diagnosis, prognosis, treatment, prescription, or formal and individualized advice from a veterinary medical professional. Animals exhibiting signs and symptoms of distress should be seen by a veterinarian immediately. |


Be the first to comment