Occurrence
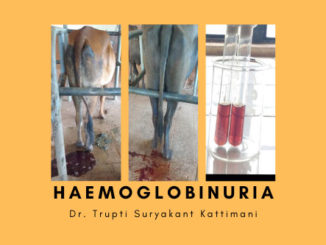
Postpartum Uterine Prolapse/ Eversion of Uterus in bovines occurs most commonly in cows immediately after parturition /occasionally upto several hours or days after wards.
Syn. Casting of “Wethers” or casting of the ‘calf bed’
Incidence: More common in Pleuripara than in Primipara
Etiology
- Hypocalcaemia
- Confinement of cow during pregnancy with its rear part sloping downwards.
- Violent tenesmus
- Relaxed, flaccid and atomic uterus.
- Retention of fetal membranes especially at the tubal and of gravid horn
- Consumption of estrogenic pasture like sweet Clover in Australia.
- Excessive relaxation of the pelvic and perineal regions
- Inadeqaute exercise.
- Vigorous forced traction applied during extraction of fetus.
- Dystocia & forceful extraction of fetus
- A low plane of nutrition may be a pre-disposing factor.
Clinical sign’s
- Symptoms may vary with the severity of the case and duration of time for which the prolapsed uterus is exposed unattended in the external environment.
- In general the animal is usually recumbent but may be in standing position with uterus hanging at the level of hocks.
- The placenta is usually retained but in other cases mucus membrane of the uterus is exposed edematous and soiled with passage of time.
- In fresh (recent) case, prolapsed mass is warm to touch but later become cold and discoloured
- The uterus may be lacerated and grossly contaminated, and mucous membrane may be enlarged and oedematous and uterine mucosa with its caruncles remains exposed.
- In cow the gravid horn is seen to be prolapsed sufficiently whereas nongravid horn is held inside.
- In most cases, prolapse of uterus leads to restlessness, pain, anxiety, anorexia, mild to moderate signs of tenesmus, increased pulse and respiration rate.
- In some cases death may occurs as a results of internal haemorrhages due to excessive tension placed on arteries by the prolapsed mass causing rupture of the uterine vessel.
Prognosis
- Prognosis of the uterine prolapse varies greatly.
- The prognosis is fairly good if the affected cow is promptly attended and prolapse is corrected.
- When uterus is severely traumatized and lacerated with profuse haemorrhage the prognosis is extremely grave.
Guidelines for the correction and replacement of postpartum uterine prolapse
- The general guideline for the correction and replacement of the prolapse of uterus is same as in case of prolapse of vagina.
- The prolapsed uterus should be initially cleaned properly with utmost care.
- A rough handling during cleaning & subsequent reduction may lead to trauma and haemorrhage. After cleaning, the prolapsed uterus is smeared with antiseptic cream.
- If there is excessive edematous condition of the prolapsed uterus then the edema may be reduced to some extent with the application of either of the following:
- Cold water/ice cubes
- Application of sterile sugar
- Injection of oxytocin
- Use of relevant herbal medicine (Prolapse in powder) pop in spray.
- It all depends upon the vet’s choice & experience. But it is needless to mention that none of these approach is widely acceptable.
- If placenta is adhered to the caruncles a gentle attempt is made to remove the placenta (F.M.). In case it is likely to produce trauma and haemorrhage the placenta is left as such.
- Posterior epidural anesthesia is helpful to avoid straining. The drugs like xylocain 2% (lignocaineHCl etc.) are widely used for epidural anesthesia.
- The prolapsed part is slowly pushed inside with due care while handling the exposed uterine mucus membrane.
- After reduction the lips of the vulva is either sutured on the hair line or truss is applied.
- It is desired that both truss and hairline suture on the vulva are applied on the same side.
- A complete course of antibiotic is given to prevent infection.
- The suture is subsequently removed when the condition seems normal.
Therapeutic Management of postpartum uterine prolapse
Principle of prolapse 3R; Reduction, Reposition and Retention
1. Replacement of uterus-3 R
- Caudal epidural anesthesia is helpful to avoid straining. The drugs like xylocain 2% 5-8 ml (lignocaineHCl etc.) are widely used for epidural anesthesia.
- The Uterus should be supported by clean towel at the level of vulva or ischial arch.
- Clean & Wash the uterus with water containing mild antiseptic (Potassium permanganate 1: 10,000) soln.
- Remove the parts of fetal membranes from the caruncles – if it separates easily, if not leave it (attached) as such.
- Repair any gross damage such as tearing by using an absorbable suture (Chromic catgut etc).
- Prolapsed mass should be raised dorsally to reduce the obstruction in urethra (Sharp Kink), resulting into removal of urine which facilitates in the reduction of the size of urinary bladder and thus prolapsed mass can easily be replaced or if by this method bladder is not reduced in size, remove the urine by using urinary catheter or aspirate the urine with the help of a fine needle.
- Replace the uterus little by little initially with those portions nearest to the vulvar lips. First the ventral portion and then the dorsal portion of the prolapsed mass should be replaced.
- During replacement of the uterus, pressure should be exerted with the help of palm and extended fingers to avoid injury to the uterus because if accidentally caruncles get ruptured, profuse bleeding may occur.
- As the prolapsed mass comes inside the vulval lips, use fist to press the prolapsed mass through the cervix to the full length of arm until the gravid horn becomes straight and no invagination remains left.
- If invagination is still present, hold the “wine bottle” with its neck & insert the hand and press the invaginated portion.
- During pressing the clenched fist, cervix should be pulled toward him or herself with one hand.
- As soon as the uterus is replaced, the hand should be kept in the uterus and the assistant should be instructed to inject 20-30I.U. Oxytocin I/M. This will facilitates the contractions of uterus and cervix. When the cervix starts contracting, the hand should be removed. In difficult / Chronic cases Buhner’s method is used after replacing the prolapsed portion.
Buhner’s Method
- Make two horizontal incisions in the perineum just below the ventral commissure and above the dorsal commissure of vulva but below the anus. (half way between the vulva and anus).
- Grasp the vulva with one hand and introduce the Buhner’s needle through the ventral incision deeply along one side of the vulva which comes out through the dorsal incision.
- Thread the Buhner tape through the eye of the needle.Forcefully pull the needle and tape ventrally, exitting through the ventral incision and remove the needle from the suture. Repeat the procedure on the opposite side of the vulva.
- Apply traction to the both ends of the suture tape to reduce the vulvar lumen so that it can accommodate only one or two fingers.
- Tie the ends of the suture tape in either a square knot or quick release knot.
- Advantage of Buhner’s method are that it is the most physiological method of retention of prolapsed mass because the suture mimics the constrictor vestibuli muscle and there is minimal deformation of vulva.
- If the animal continues straining following replacement of the uterus, it may be due to invagination of the tubal end of uterine horn or an irritation or inflammation of the vulva.
- The invagination can be corrected by inserting the clenched fist again. The irritation can be abolished by applying the xylocaine jelly (2 % Lingocanine Jelly) on the vulva.
2. Post replacement therapy
- Antibiotics like oxytetracycline for 5 to 7 days.
- NonSteroidalAntiinflammatory drugs (NSAIDS)Meloxicam/Maxtal15-30 ml I/M.,
- Anti-histaminics –Chlorpheniramine maleate / Pheniramine maleate 10 ml I/M.,
- Inj. Vitamin B-complex – Beekom –L / Pepcid For 5 day I/M.,
- Tranquillizers – like Sequil- 5 ml I/M.,
- Intra-uterine antibiotic/antimicrobial for 3-5 days.
- Application of xylocaine jelly on the vaginal wall 2 to 3 times for 3 to 5 days.
Advice to the owner
- Good Nursing
- Laxative diet.
- Moderate exercise
- Rear portion of the animal should be raised.
| The content of the articles are accurate and true to the best of the author’s knowledge. It is not meant to substitute for diagnosis, prognosis, treatment, prescription, or formal and individualized advice from a veterinary medical professional. Animals exhibiting signs and symptoms of distress should be seen by a veterinarian immediately. |


Be the first to comment